01 - The problem
The problem isn't translation. It's loss of autonomy over your own healthcare.
When you ask a Spanish speaker in Germany what frustrates them about the healthcare system, the most common answer is "I don't understand medical German." That's the surface answer. The real problem is continuous: people lose autonomy over their own care. Not because information doesn't exist, but because they lack actionable comprehension, the judgment to navigate the system, and a presence that reduces fear. The loss of autonomy hits hardest when there are children or elderly parents in the family.
I ran 11 in-depth interviews across 4 German cities. The key finding: fear drives usage, not curiosity. People don't use this kind of product to learn. They use it to reduce anxiety. The highest willingness to engage came around children's health, then elderly parents. Another finding: WhatsApp is the natural channel. When someone finishes at the doctor with a paper they don't understand, they open WhatsApp to complain to their mom. Not the browser.
02 - Discovery
11 interviews, 4 cities, 6 weeks of regulatory reading
Before designing anything, I spent 6 weeks on three parallel tracks. 11 deep interviews with Spanish speakers in Germany (ages 28 to 67, residence times 2 to 22 years). Long conversations with the two physicians on the team to understand what questions they get from Spanish-speaking friends, most of which aren't medical consultations but comprehension requests. And a deep read of relevant German regulation: Heilpraktikergesetz, MDR, DSGVO applied to health data, Bundesärztekammer guidelines on Fernbehandlung.
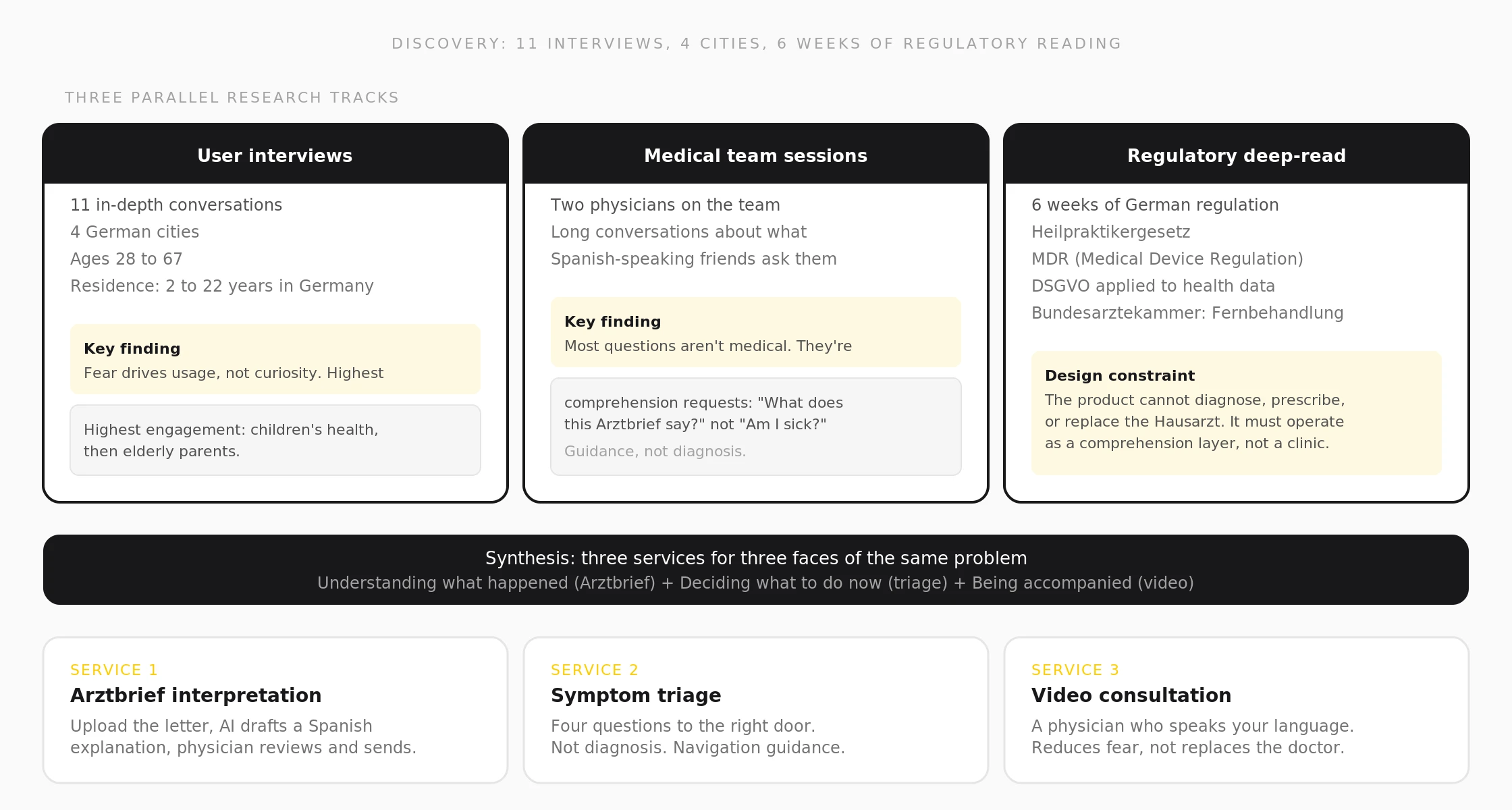
Three parallel research tracks. User interviews (11 conversations, 4 cities), medical team sessions (comprehension vs. diagnosis), and 6 weeks of German healthcare regulation.
03 - Strategic decisions
Six decisions that hold the whole product together
1. The golden rule: physicians don't operate channels. Dr. David Sánchez, médico colombiano con Approbation alemana y enfoque en medicina interna, and Dra. Juliana Henríquez, médica colombiana con Approbation alemana y enfoque en pediatría, both work full-time in clinics. I operate all channels. They appear in two fixed weekly 20-minute video consultation slots each.
2. Controlled capacity with an explicit ceiling. Maximum 20 new users per week. A quality decision, not a technical limitation. When the queue fills, new users join a waitlist with a specific date.
3. AI proposes, human physician decides. The AI layer (Claude with vision on the Arztbrief) generates a structured draft in four blocks. Only when model confidence is high and no critical keywords are detected (Karzinom, Tumor, Myokardinfarkt, and 40+ others) does the system auto-send. Otherwise, the case queues for human review.
4. Disclaimers are interface, not footer. Each response includes a clear disclaimer: no diagnosis, no prescription, in emergencies call 112. Integrated into the flow, visible, with a tone of care rather than fine print.
5. The product voice: care without paternalism. No "don't worry." No diminutives. No unnecessary jargon. Every response has four fixed blocks: what your Arztbrief says, what it means, what to do now, what to ask next time.
6. Deliberate bilingualism. User-facing product 100% Spanish. Internal documents in parallel German-Spanish columns. The layer facing the German system speaks German. The layer facing the user speaks Spanish.
Every decision came from the research, not from assumptions. The capacity ceiling (20 users/week) came from the physicians' real availability. The AI confidence threshold came from testing the Arztbrief interpretation against 50 real documents and finding the failure modes. The product voice ("care without paternalism") came from the interviews: users were exhausted by condescending health content. Each decision traced back to a specific finding. Nothing was designed from first principles alone.
04 - The MVP
Three services, three channels, one coherent product
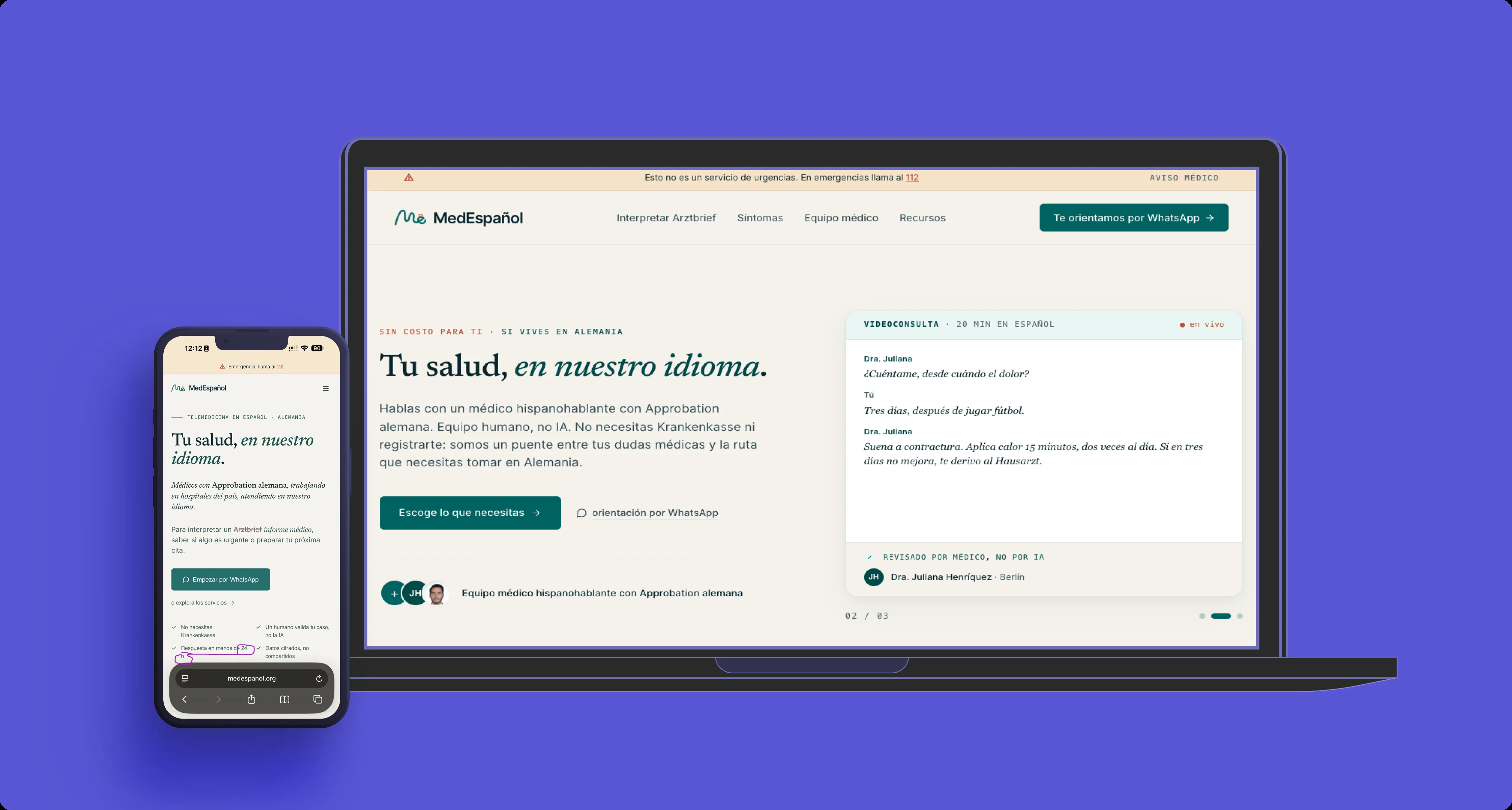
The MVP shipped with Arztbrief interpretation (upload photo or PDF, AI draft with human review, response via WhatsApp), symptom triage (4-step wizard: Hausarzt, Bereitschaftsdienst 116 117, Notaufnahme, or 112), and 20-minute video consultations in Spanish with physicians with German Approbation. Plus an admin panel (/admin) for case management, physician workload caps, and impact tracking.
Stack: Next.js 14, TypeScript, Tailwind with custom tokens, Supabase (Postgres + RLS), Claude API (Anthropic), Resend, Cal.eu, WhatsApp Business, Vercel.
Symptom triage wizard. Four questions to the right door. Navigation guidance, not diagnosis.
Arztbrief interpretation. Upload the letter, AI drafts a Spanish explanation, physician reviews and sends.
Admin panel. Case management, workload caps at 20 users/week, and impact tracking for the medical team.
05 - Process artifacts
Built directly in code, no Figma file for this one
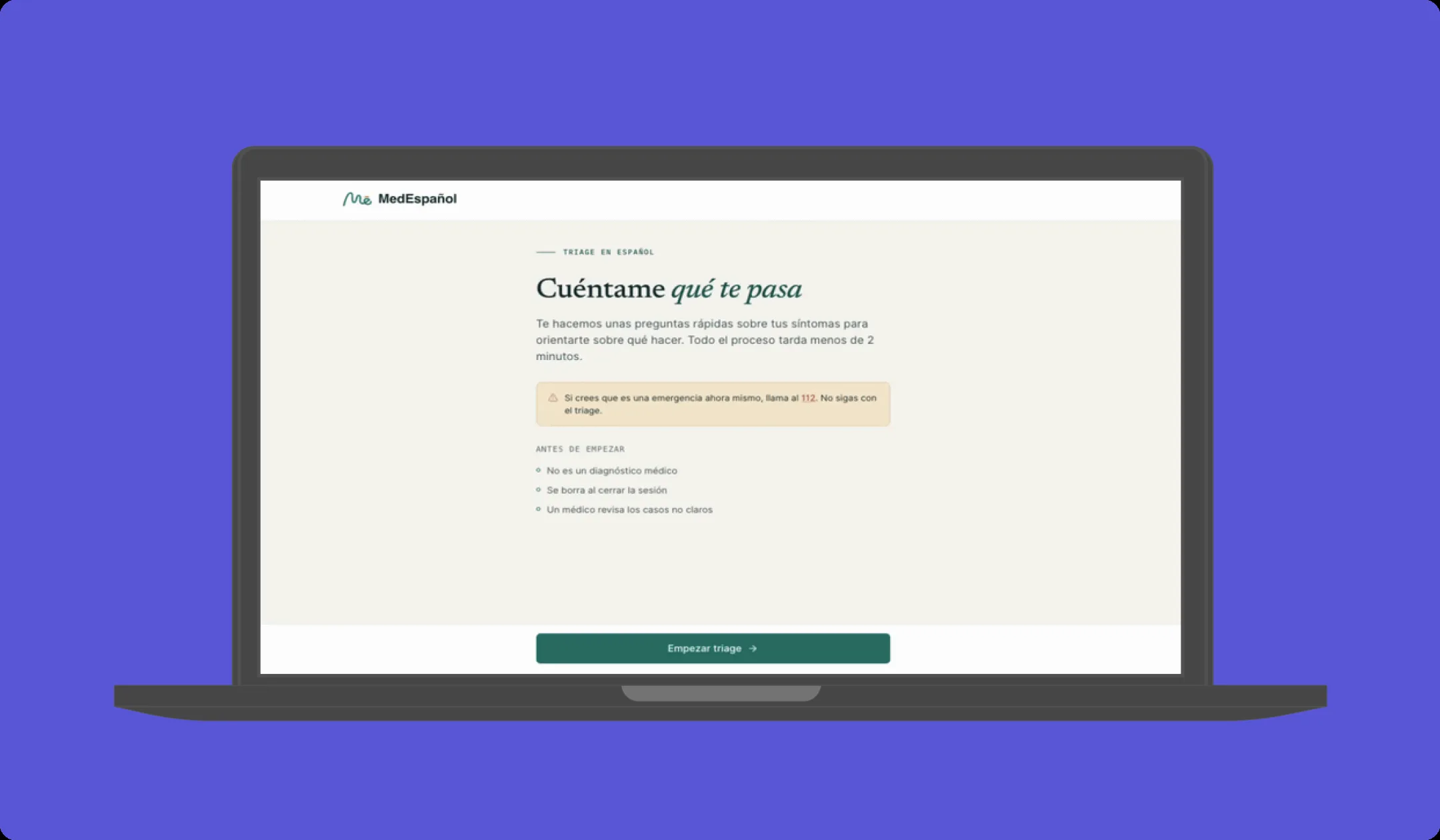
Triage flow. Each question narrows the recommendation. Urgent cases route to 112, non-urgent to the right specialist type.
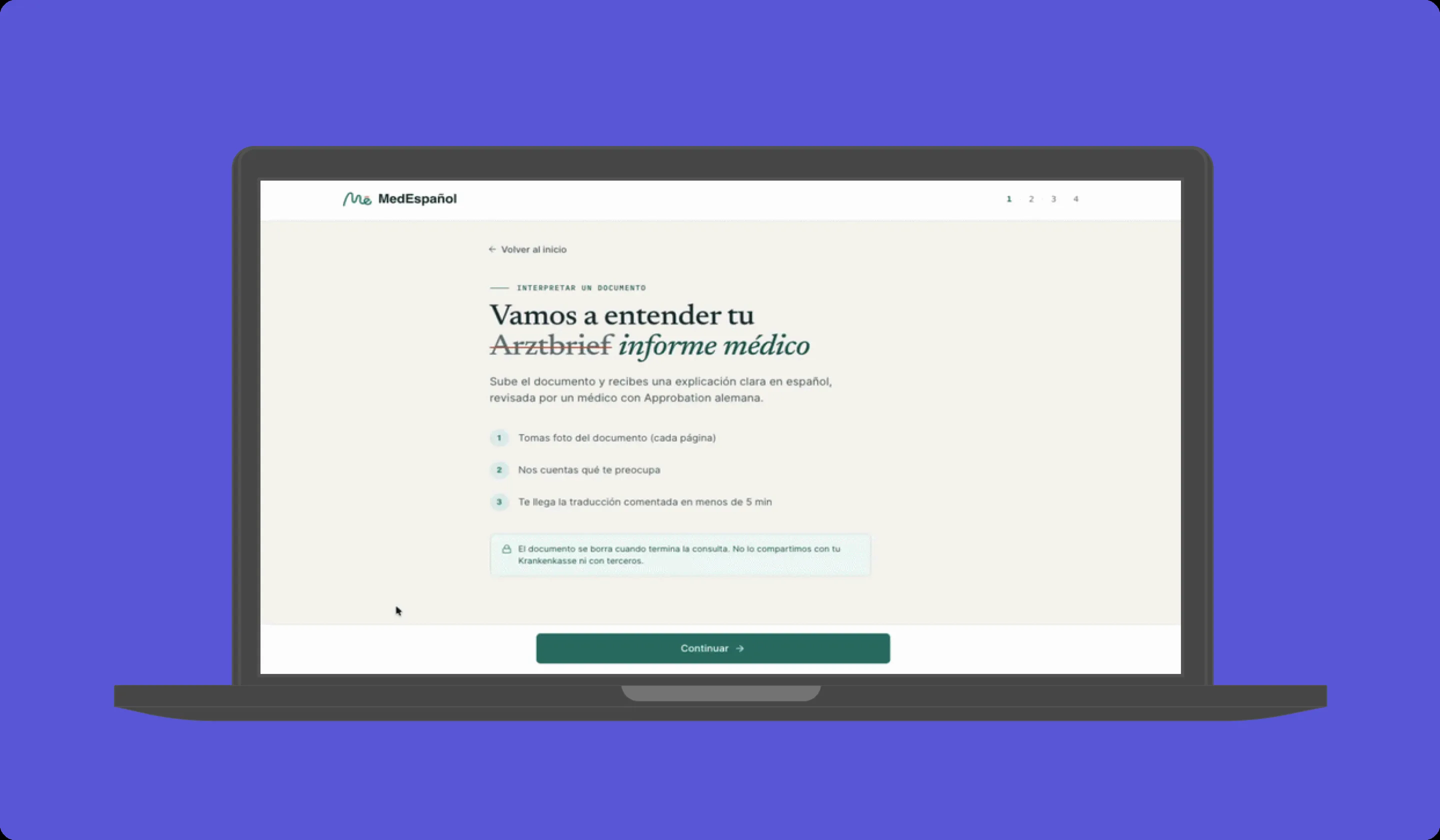
Arztbrief flow. AI proposes, physician decides. Auto-send only when confidence is high and no critical keywords detected.
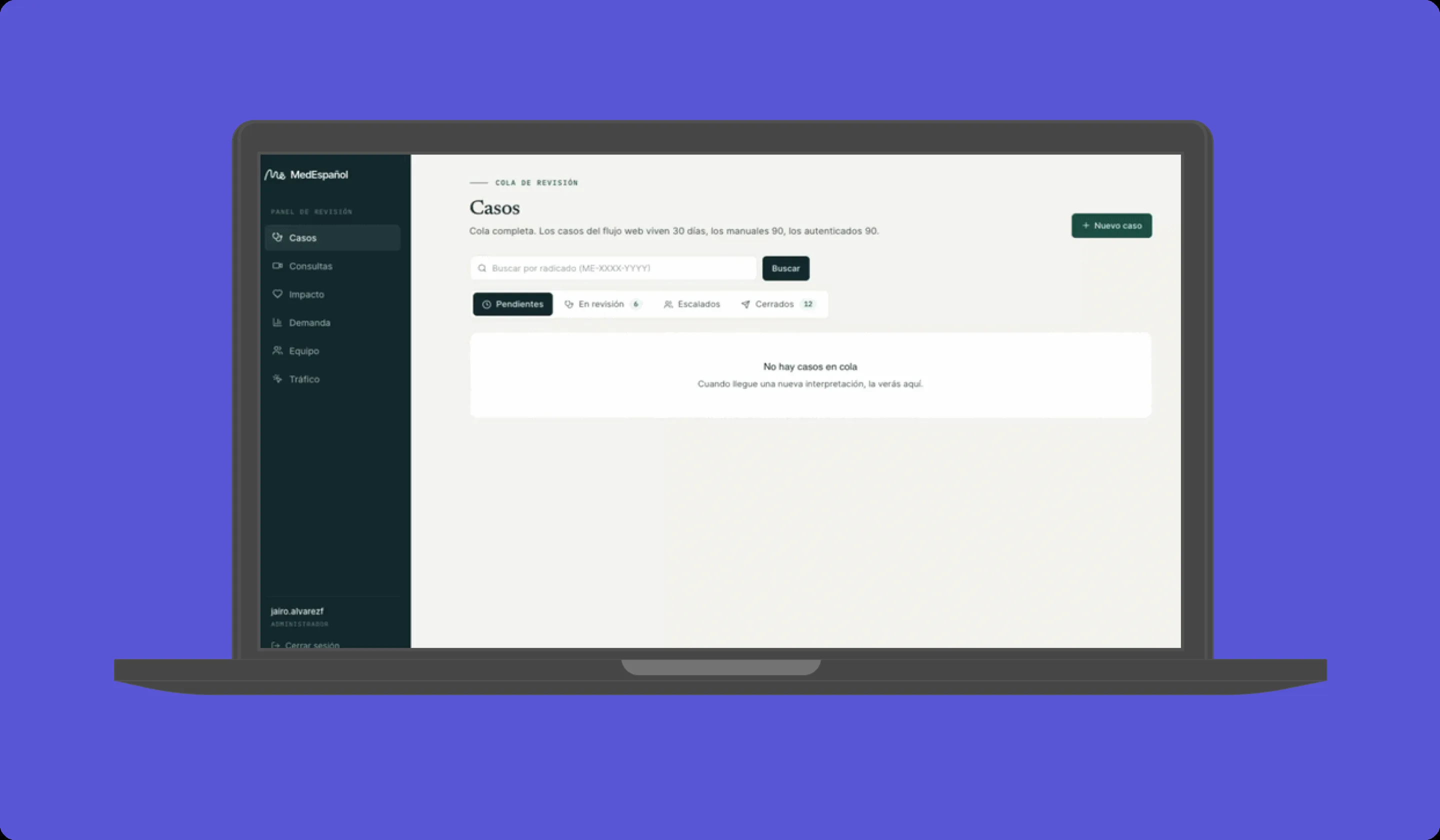
Operations view. Physicians don't operate channels. The admin layer handles scheduling, capacity, and routing.
06 - The solution
A guidance layer, not a replacement for the Hausarzt
MedEspañol operates as a comprehension and navigation layer. It doesn't diagnose, prescribe, or replace emergency services. Three services cover the three practical faces of the problem: understanding what already happened (Arztbrief), deciding what to do now (triage), and being accompanied by someone who speaks your language (video consultation). The product captures demand for uncovered areas (gynecology, mental health, dermatology) through a form, without promising service.
07 - What I learned
Building alone taught me what I actually know
I made every product, design, architecture, and compliance decision. No team to delegate to. When the Arztbrief flow broke at 2am, I fixed it. When a regulatory question came up, I read the law. When the physicians needed a panel that respected their time constraints, I built it. Five weeks from zero to production, without a prior codebase and without an engineering team. The constraint forced clarity: if I can't explain why this feature exists in one sentence, it doesn't ship.
The research phase shaped every design decision that followed. The 11 interviews didn't just validate demand. They defined the product voice (care without paternalism), the primary channel (WhatsApp, not browser), the capacity model (20 users/week ceiling), and the regulatory boundaries (guidance layer, not clinic). Without those 6 weeks of discovery, the product would have been a translation tool instead of a healthcare navigation service.
08 - What I chose not to build
Deliberate omissions that protect the model
1. Live consultation accompaniment (interpreter during medical appointments). The most differentiating feature and the most expensive to build well. Requires medical consent protocol, assisted transcription with strict privacy, different architecture. Roadmap phase 2.
2. User cloud history. Useful but not critical to validate the core problem. Would complicate DSGVO from day one. Phase 2 as premium feature.
3. Native mobile app. WhatsApp already covers the channel. Building native would double development without proportional value delivery.
4. Payment in the MVP. Charging in the first 6 months introduces bias in metrics and dilutes feedback. Deferred until institutional funding path is clear.